
This past year, The Economist published a series of Six Big Ideas that define economics today. One piece, entitled Two out of Three Ain’t Bad, discussed the macroeconomic concept of the trilemma. The article begins:
Hillel the Elder, a first-century religious leader, was asked to summarize the Torah while standing on one leg. “That which is hateful to you, do not do to your fellow. That is the whole Torah; the rest is commentary,” he replied. Michael Klein, of Tufts University, has written that the insights of international macroeconomics (the study of trade, the balance-of-payments, exchange rates and so on) might be similarly distilled: “Governments face the policy trilemma; the rest is commentary.”
In the field of macroeconomics, policy makers must understand the complicated relationships between interest rates, exchange rates, and capital flows. The self-interested decisions made by countries impact the economies of others. Fortunately, medicine is much simpler.
In a previous posting, I discussed the operational priorities of cost, quality, timeliness, and flexibility. If we substitute the term “access” to represent a combination of timeliness and flexibility, we can construct a similar trilemma for medicine. This medical trilemma would consist of cost, quality, and access. It would look something like this:
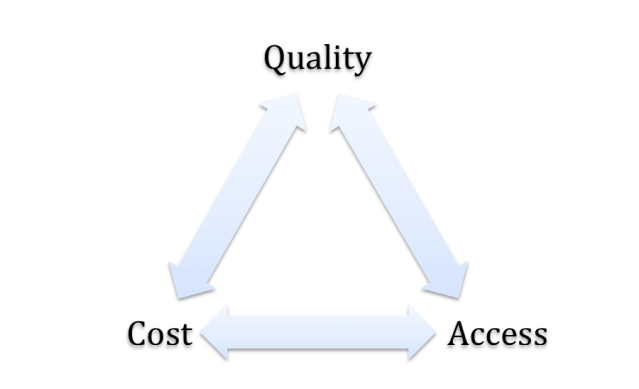
The key to a trilemma is that an operator must pick one side of the triangle to operate along. The operational priority at the third point cannot be directly influenced; it is a dependent variable that only responds to inputs from the chosen side of the trilemma.
A medical trilemma could unify and support discussions regarding operations in medicine. Much of the debate in health care today argues one of these points in isolation, which is reductionistic, noisy, and fails to produce sustainable solutions.
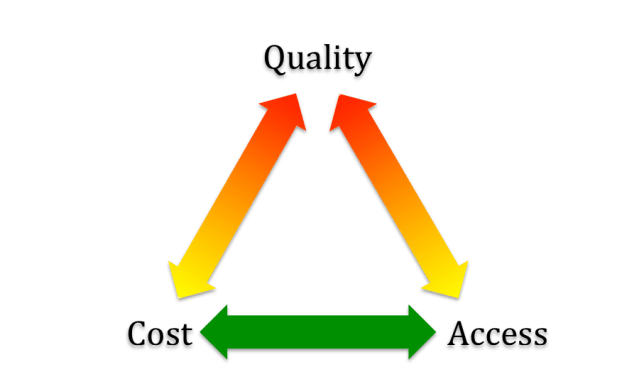
If viewed through the lens of the trilemma, it becomes clear that that we need to focus on costs and access. The increasing financial burden that Americans spend on healthcare is already unsustainable; it continues to consume up to an unhealthy 20% of GDP. Within families, difficult choices must be made with limited resources. On a national scale, this healthcare expense siphons money away from our schools, defense, and infrastructure. Costs must be contained, and there is increasing awareness within radiology that perhaps costs have been ignored for too long.
Regarding access, the demographics of the health care consumer are not favorable. By now we should all be familiar with the concept of our aging population and the fact that demand for healthcare is likely to outstrip supply in the coming decades. So where does that leave quality? I believe that quality will be the dependent variable left to float.
I am not suggesting we enact “death panels” or anything that inflammatory. I am simply suggesting that future gains in quality must be viewed through the lenses and operational priorities of cost and access. We must focus on operating along the base of the depicted trilemma given our current American demographic and financial tensions.
For example, many pharmaceutical companies are currently developing personalized medicine solutions regardless of expense. This strategy may not be sustainable in the long run. A $250,000 immunotherapy that yields a few additional weeks of sickness would not be supported by this trilemma.
Given the constraints in America today, two out of three is not bad. In the future, perhaps we will apply this model to other examples in medicine and decide what is important and what is noisy “commentary”.

Pingback: Reviving a Classic Model in Medicine – Seth M. Hardy, MD
Pingback: Lung Cancer Screening’s Five Forces – Seth M. Hardy, MD
Pingback: Time For A Expanded Mission At The CDC – Seth M. Hardy, MD MBA
Pingback: It’s (Still) the Prices, Stupid | Health Advice and more